Does the flu shot produce any effect to limit or mitigate contracting influenza? Does the flu shot reduce the risk of COVID-19? Let us briefly answer these two questions here with studies and pharmaceutical company leaflets.
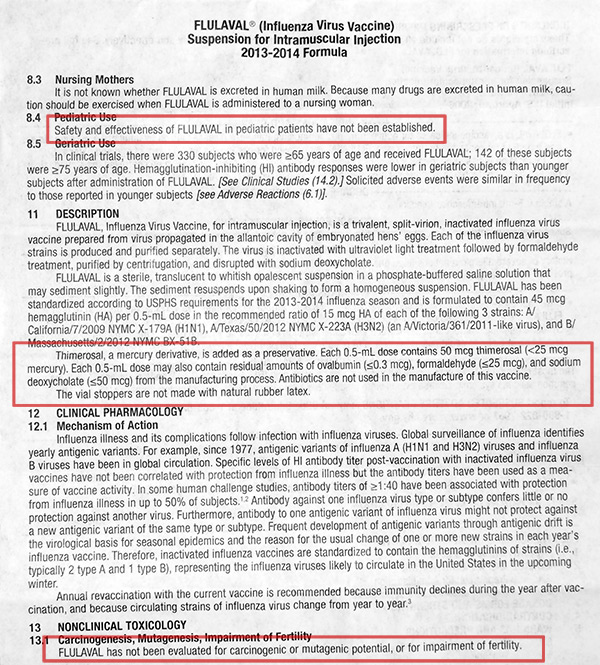
There have been many who have refuted the benefit of taking a flu shot. To the point of these practitioners calling the flu shot a fraud. But this fraud is said to be deeply embedded in the delusional pro-vaccine culture of the pharma-controlled medical industry that even well-meaning doctors and pharmacists (who are otherwise very intelligent) fail to realise flu shots don’t work. By only going by what is read in a leaflet, the flu shot vaccine inserts openly admit there is no scientific evidence demonstrating flu shots prevent the flu.

People who receive the flu shot almost never receive the insert sheet. It’s not handed out by doctors and pharmacists because either don’t know themselves or they don’t want people to realize the extent of the pseudoscience behind the flu shot fraud. In fact, most people who have taken flu shots, and I was one of them many years ago, aren’t even aware that an insert sheet exists at all. Furthermore, GlaxoSmithKline confirms there is no evidence to back this flu shot.
COVID-19 mortality rate in Italy and the flu vaccine
In case you are not aware, the infection rate mortality rate in Italy to COVID-19 is dramatically higher. Why? Well the standard answers of an elderly population and the failure to implement social distancing soon enough just don’t explain what is happening. Dr. Alex Vazquez, who Dr Murray refers too in his newsletter to the public, provides valuable insight.
Dr. Alex Vazquez states that in September 2019, Italy rolled out an entirely new type of influenza vaccine. This vaccine called VIQCC is different than others. Most available influenza vaccines are produced in embryonated chicken eggs. VIQCC, however, is produced from cultured animal cells rather than eggs and has more of a “boost” to the immune system as a result. VIQCC also contains four types of viruses – 2 type A viruses (H1N1 and H3N2) and 2 type B viruses.2 It looks like this “super” vaccine impacted the immune system in such a way to increase coronavirus infection through virus interference that set the stage for what happened in Italy.
A study published in the journal Vaccine, a peer-reviewed medical journal, published by Elsevier, titled Influenza vaccination and respiratory virus interference among Department of Defense personnel during the 2017-2018 influenza season, reveals that influenza vaccination may increase the risk of infection from other respiratory viruses — the phenomenon described above as virus interference. The study compared the respiratory virus status among 2,880 Department of Defense personnel based on their influenza vaccination status demonstrated. The virus interference phenomenon goes against the basic assumption of the test-negative vaccine effectiveness study that vaccination does not change the risk of infection with other respiratory illness, thus potentially biasing vaccine effectiveness results in the positive direction. The study concluded “Vaccine derived virus interference was significantly associated with coronavirus.”
.jpg)
The study results contradict what the medical profession, that of the medical aid companies and those of a recent health recommendation that one should get an influenza vaccine to protect against Coronavirus-19.

A 36% and 51% increased risk of coronavirus and human metapneumovirus in influenza vaccinated individuals, was shown respectively. You can research more however be aware of the risk of taking a flu shot, coronavirus or not.

Encourage your clients to get a flu vaccine – Medical Aid to Advisor
The largest medical aid scheme in the country sent out an email to advisors to encourage clients to go for a flu vaccine during COVID-19. Given the risks involved in this and not informing you of the potentail risk, could place you at a greater risk of infection. Given our risk-managed approach to health and life, I would err on the side of caution when it comes to vaccines, and specifically for the flu vaccine and it’s benefit for nCoV-19.
There is no more important time than now during the current COVID-19 pandemic, to ensure that clients with specific conditions who are considered to be at higher risk of complications for COVID-19, need to take extra preventive measures and precautions during this time to avoid contracting this illness. Since the flu season and COVID-19 are now overlapping, the National Institute for Communicable Diseases (NICD) in South Africa has recommended that everyone, in particular those who are at high-risk of developing severe flu and flu-related complications, receive a flu vaccination ahead of influenza season this year. To receive the full benefits of the vaccine, your clients ideally need to get vaccinated before the flu season begins during March or early April as the vaccine is already available.
Medical Aid in South Africa
Vaccine propoganda and the best solution?
We have come to learn that with the attempt to create a vaccine for SARS-CoV, that vaccines were able to offer protection against infection, but came with a cost of disruption to the immune system. This altered immune function led to severe lung inflammation when test animals were exposed to the virus. The final statement of the study cannot be highlighted enough: “Caution in proceeding to application of a SARS-CoV vaccine in humans is indicated.” 3
Certain medications increase risk for infection and mortality?
The body responds to ACE inhibitor drugs used in the treatment of high blood pressure by increasing the number of ACE-2 receptors on cells. With an increase in ACE-2 receptors there are more entry points (doors) that the SAR-CoV-2 virus can enter the cell.5
The secondary route of infection for many respiratory tract viruses like SAR-CoV-2 is through the gastrointestinal tract. Interestingly, this ability of a coronaviruses to travel from the gut to the lungs was confirmed with Middle East respiratory syndrome coronavirus (MERS-CoV) by increasing the gastrointestinal replication of the virus by infecting animals with viruses orally while at the same time giving them an acid-blocking drug known as a proton pump inhibitor.6 This class of drugs includes Nexium, Prilosec, Protonix, Prevacid, and Aciphex. So, to answer to the obvious question “Does taking a proton pump inhibitor increase the risk for COVID-10 that can attack the lungs by increasing the secondary route of access to the lungs.” The answer is a resounding YES!
Is it chloroquine or is it zinc that is working as a possible aid in treating COVID-19? No it is Vitamin C
Chloroquine is a drug long used to treat malaria. Hydroxychloroquine is a closely related compound that has also been used to treat malaria, but more recently has been used to treat autoimmune conditions such as lupus and rheumatoid arthritis.
More recently these drugs have been shown in vitro (in a test tube, not a living organism) to have a broad spectrum of antiviral activities. Although they have never been shown to have clear antiviral activity in humans against any virus, they have become widely used in China to treat COVID-19.
The potential of these drugs to treat COVID-19 received a lot of hype from Donald Trump recently. As a result, out of fear of the virus and hype over chloroquine, a Phoenix man and his wife drank a fish tank cleaner containing chloroquine phosphate. The man died and the wife wound up in critical care.
As reviewed in “Of Chloroquine and COVID-19,”
“To date, no acute virus infection has been successfully treated by chloroquine in humans.” It failed to treat flu or dengue in humans.
For chronic viruses, the results in HIV have been inconclusive, and the results with hepatitis C have been so slight that it’s never become part of a standard protocol.
Although chloroquine has been shown to be antiviral in vitro against SARS-CoV-2, the cause of COVID-19, it also proved antiviral in vitro against chikungunya virus, yet acted as a proviral in living mice. This might be because it can suppress the immune system and might relate to the effectiveness of hydroxychloroquine as a treatment for autoimmune disorders. Could it also make COVID-19 worse?
Despite the widespread use of chloroquine and hydroxychloroquine to treat COVID-19, there are as yet no randomized controlled trials clearly showing it is effective.
A “Systematic Review on the Efficacy and Safety of Chloroquine for the Treatment of COVID-19” suggested similar caution. The authors performed a comprehensive search for everything related to the topic and found very little that had already been published: an in vitro study, two letters, a consensus panel of Chinese experts, a Dutch national guideline, and an Italian national guideline. 23 Chinese trials had been registered, but as of March 10 when this was published, none of the data had been released.
That the expert opinion was running far ahead of the data is demonstrated in this quote from the paper:
A narrative letter by Chinese authors reported that a news briefing from the State Council of China had indicated that “Chloroquine phosphate… had demonstrated marked efficacy and acceptable safety in treating COVID-19 associated pneumonia in multicentre clinical trials conducted in China.” The authors also stated that these findings came from “more than 100 patients” included in the trials. Evidence of such data in the trial registries was not found by the researcher.
Review of a non-randomized French trial of hydroxychloroquine suggested the drug virologically cured 15 out of 26 people, while it nauseated one, put three in ICU, and killed one. Because it wasn’t randomized, it isn’t clear whether the cure or the worsening represent true effects of the drug, but if we are to regard the cure as a real effect, we also have to regard the worsening as a real effect, suggesting that if it works it might have a high risk profile
The World Health Organization is launching a multinational set of trials testing the efficacy of interferon, chloroquine, lopinavir, and ritonavir. This should provide us with some information, but right now a lot of things are being thrown at COVID-19 with no clear evidence they are effective.
That WHO is launching this trial should also help allay rational fears that Chinese data can’t be trusted. After all, China just expelled all the American journalists, so it’s clear the Chinese government doesn’t value transparency around the COVID-19 situation.
So, are hydroxychloroquine or chloroquine effective?
It could be a 50/50 bet, at best.
Plant polyphenols and flavonoids act to increase the antiviral effects of zinc?
Flavonoids are a group of plant pigments largely responsible for the colors of many fruits and flowers. As a class of compounds, flavonoids have been referred to as “nature’s biologic response modifiers” because of their ability to modify the body’s reaction to viruses, allergens, and carcinogens. Quercetin is generally the most powerful of the flavonoids in cellular studies, but it is poorly absorbed. Quercetin is a zinc ionophore that is about 35% as strong as chloroquine, but unlike this drug that can have serious side effects, quercetin is completely safe.7
Quercetin is available alone in powder, tablet, and capsule form as well as in beverages. However, since quercetin is poorly absorbed. For this important action as a zinc ionophore to fight SARS-CoV-2, it is best to use the phytosome form of quercetin. This form involves binding quercetin to phosphatidylcholine from sunflower lecithin through a patented process to improve absorption. It has been said that the blood level of quercetin produced by the phytosome form is greater than 50 times the level produced by an equal amount of regular quercetin. Hence, 250 mg of quercetin phytosome providing 100 mg of quercetin would be equivalent to 5,000 mg of quercetin.
Vitamin C in Wuhan and globally for all coronavirus’
I also find it ironic that many people will beat the “trust the experts” drum endlessly, bashing anyone suggesting nutrients or herbs could be relevant, yet vitamin C, D, elderberry, and garlic have all been shown to have antiviral effects in humans, yet hydroxychloroquine and chloroquine have not. Why do these drugs get special status just because the experts are using them with no evidence of their efficacy? Following the work on the ground in Wuhan and what has happened, vitamin C therapy has produced outstanding results. See our previous article on vitamin C therapy in Wuhan.
References:
- Wolff GG. Influenza Vaccination and Respiratory Virus Interference Among Department of Defense Personnel During the 2017-2018 Influenza Season. Vaccine 2020;38 (2):350-354.
- https://www.doctorsinitaly.com/b/flu-shot/
- Tseng et al. Immunization With SARS Coronavirus Vaccines Leads to Pulmonary Immunopathology on Challenge With the SARS Virus. PLoS One 2012;7 (4): e35421.
- https://www.drugtargetreview.com/news/57834/preliminary-sars-cov-2-protease-inhibitor-shows-efficacy-in-mice/
- https://www.sciencedaily.com/releases/2020/03/200323101354.htm
- Zhou J, Li C, Zhao G, et al. Human intestinal tract serves as an alternative infection route for Middle East respiratory syndrome coronavirus. Sci Adv. 2017 Nov 15;3(11):eaao4966.
- Dabbagh-Bazarbachi H, et al. Zinc ionophore activity of quercetin and epigallocatechin-gallate: from Hepa 1-6 cells to a liposome model. J Agric Food Chem. 2014 Aug 13;62(32):8085-93.
- Riva A, et al. Improved Oral Absorption of Quercetin from Quercetin Phytosome®, a New Delivery System Based on Food Grade Lecithin. Eur J Drug Metab Pharmacokinet. 2019 Apr;44(2):169-177.
- https://www.sciencedirect.com/science/article/pii/S0264410X19313647?via%3Dihub
- Study published in PNAS
- C Masterjohn. Can Hydroxychloroquine or Chloroquine Treat COVID-19? [COVID-19 Updates]