As Covid cases, hospitalizations, and now deaths soar in Israel even though over 90 percent of older adults are fully vaccinated, the country is aggressively pushing a third shot. Hundreds of thousands of older Israelis have already received it.
We have learned that a COVID-19 booster shot would become available the week of September 20, 2021. People 18 years and older who received the Pfizer or Moderna vaccines will be eligible for a booster dose eight months after their second dose. People who got the single-dose Johnson & Johnson vaccine would also likely need an additional shot to prolong its effectiveness against coronavirus infection and to reduce the severity of COVID-19 symptoms.
Other countries are preparing to follow. Now the inevitable is happening. The third shot is beginning to fail.

The desperate move for a third shot is the latest and maybe most desperate manifestation of the panic around the vaccine failure that health authorities still will not openly admit is happening.
And it is profoundly anti-science.
These mRNA vaccines are not Pepto-Bismol. They have profound biological effects. They are encapsulated in fat particles whose long-term effects are unknown. They spread throughout the body (despite the early promise they would not). They hijack cellular machinery in exactly the same way an actual virus does.
They are no joke.
And – as rushed and flawed as their development was last year – at least regulators forced Pfizer and Moderna to test them in large clinical trials, with a total of more than 70,000 people.
The trials had two main goals: to make sure they didn’t have massive, immediate side effects (safety) and that they actually worked against the virus (efficacy).
In fact, the trials showed the vaccines did have a nasty short-term side effect profile – and that it worsened after the second dose. And despite their size, the trials failed to catch severe side effects for both the mRNA vaccines (which – at the least – cause heart inflammation in some young people) and the Johnson & Johnson and AstraZeneca vaccines, which cause a rare but particularly nasty form of blood clotting.
Still, most side effects appeared to fade after a few days. The trials also showed that at peak protection after the second dose, the mRNA vaccines reduced infections by 95 percent.
Thus their almost immediate authorization.
—
But now we know better.
The real-world data – from Israel, the United States, and everywhere else – are clear. Protection from infection fades within months even against the original coronavirus. It shrinks essentially to zero against the Delta variant (we can argue about time vs. variant effects, but the answer doesn’t matter in this context, either way the vaccines have stopped working).
For now, vaccine advocates are clinging to the hope that even if the vaccines do not protect against infection, they still provide some protection against more serious illness and death. I think the jury is still out on that question, but again it is largely irrelevant for this conversation – the Covid wards are filling in Israel, and most people in them are older and vaccinated. If the vaccines do offer any help after a few months against serious illness, it is far less than the 95-99 percent protection that advocates have claimed.
Thus the move for a third shot. And possibly more shots to come.
But please – please! – understand how radical a move this is.
At this point, these shots are basically being pushed forward on the basis of VERY early data from VERY small trials – a few dozen volunteers, at most – showing that people had significantly more antibodies a month after receiving a third dose.
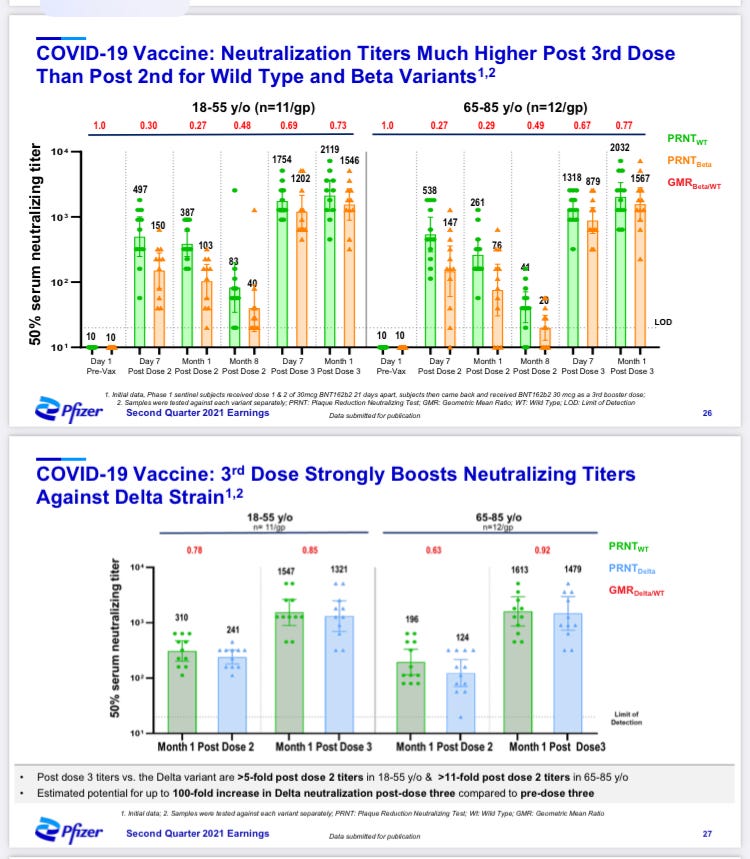
I don’t doubt these slides are accurate.
THE VACCINES MAKE YOUR CELLS PRODUCE THE SPIKE PROTEIN. YOUR BODY THEN MAKES ANTIBODIES TO THOSE PROTEINS.
That’s what they do, and they’re very good at it. More vaccine makes your body do it more.
But that’s only the beginning of what we should know before encouraging a third dose. Here’s a PARTIAL list of questions we haven’t answered:
Does a third dose of the vaccine ACTUALLY REDUCE INFECTIONS IN THOSE PEOPLE WHO RECEIVE IT?
Does it reduce deaths (remember, even the original, huge Covid trials didn’t answer that question)?
Will the third dose produce a transient spike in infections, as the first dose appears to?
Will the antibodies last longer this time because we have more of them after the second dose, or will they decline more quickly?
Does the vaccine confer ANY long-term protection through T-cell immunity?
Will people who have received a third dose be vulnerable to future variants? Will they be more or less vulnerable than people who have been infected and recovered and are are naturally immune?
Will the side effects – which are generally much worse after the second dose than the first – be still worse after the third?
Will some people die from those side effects?
What is the overall safety profile of the third or more doses in a large population?
Does it differ by age?
—
I could go on, but I hope this is enough to show you how little we know.
Offering a third dose essentially means offering an entirely new vaccine regimen. If the FDA or other regulators had any guts they would insist on a new, full-size clinical trial (a BETTER trial, one powered to detect reductions in death) before allowing it.
Instead governments are rushing ahead based on what are basically early Phase 2 clinical trials – tiny and providing evidence of efficacy based on lab benchmarks rather than clinical data.
Yet, based on the stock action in Moderna and BioNTech in the last few days, investors are VERY confident these boosters are going to be part of our lives going forward.
And so the madness continues.